I spent the first decade of my career inside health systems billing analyst, then revenue cycle director for a regional network in Dallas. The second decade I have spent working directly with independent practices, and the contrast is jarring in one specific way: large health systems have entire departments dedicated to revenue cycle management. Independent practices usually have one biller, one front-desk person, and a physician who checks the bank account on Fridays hoping the numbers make sense.
That structural gap is why revenue cycle management (RCM) is one of the most important concepts a practice owner can understand not because you need to manage it yourself, but because if you do not understand what it is, you cannot tell when it is failing you.
This guide covers what RCM actually is, the eight steps that make up the revenue cycle, where most independent practices lose money, and what a well-managed cycle looks like in practice.
What Is Revenue Cycle Management in Healthcare?
Revenue cycle management (RCM) is the end-to-end process a medical practice uses to manage the financial lifecycle of every patient encounter from the moment an appointment is scheduled to the moment final payment is posted to the practice’s account.
According to the Healthcare Financial Management Association (HFMA), revenue cycle management encompasses all administrative and clinical functions that contribute to the capture, management, and collection of patient service revenue. In plain terms: every step between ‘patient books appointment’ and ‘practice gets paid’ is part of the revenue cycle.
RCM is not just billing. Billing is one step inside a larger system. A practice with excellent coders but poor eligibility verification will still generate a high denial rate. A practice with clean claims but no AR follow-up process will still watch payments age and disappear into write-off columns. The whole cycle has to work.
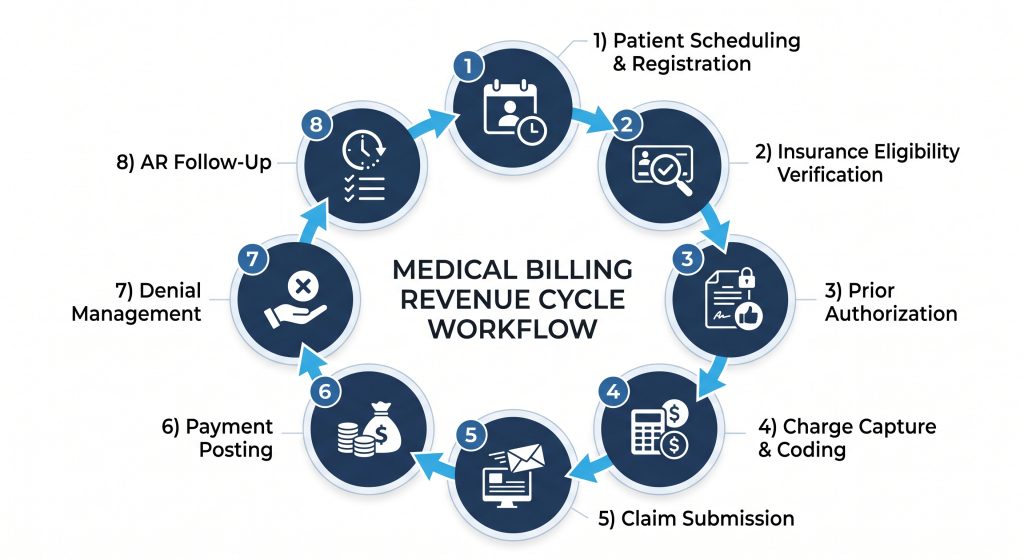
The 8 Steps of the Revenue Cycle And Where Practices Lose Money
Step 1 — Patient Scheduling and Registration
The revenue cycle starts before the patient arrives. Accurate collection of patient demographics, insurance information, and primary care referrals at the point of scheduling determines whether a claim can even be submitted correctly. Errors at registration account for roughly 23% of all claim denials, according to MGMA benchmarking data making this the single highest-leverage point for denial prevention.
Most practices treat registration as a front-desk administrative task. It is also a revenue protection task. A wrong insurance ID, a missing group number, or an outdated subscriber date of birth will produce a denial three to four weeks later, long after the patient has left and the staff member who made the error has forgotten the encounter.
Step 2 — Insurance Eligibility Verification
Before a patient is seen, the practice needs to confirm that their insurance is active, that the provider is in-network, and what the patient’s specific benefits look like — deductible, copay, coinsurance, and any specialty-specific limitations. Eligibility errors are the second most common cause of claim denials in U.S. physician practices, per CMS claims processing data.
Real-time eligibility verification through a clearinghouse takes under 30 seconds. Practices that skip it or run it only at initial registration rather than before every visit pay for it in avoidable denials and patient billing disputes at the back end.
Step 3 — Prior Authorization
Certain procedures, medications, and specialist referrals require payer approval before the service is rendered. Providing a service without obtaining required prior authorization is one of the most expensive mistakes in the revenue cycle the resulting denial is typically non-appealable.
The AMA’s 2023 Prior Authorization Physician Survey found that 94% of physicians report prior authorization causes treatment delays, and practices spend an average of 13 hours per physician per week on prior authorization tasks. For a small practice, that is a significant administrative burden with zero revenue attached to it.
Step 4 — Charge Capture and Medical Coding
After a patient visit, the clinical documentation is translated into billable codes CPT codes for procedures and services, ICD-10-CM codes for diagnoses, and HCPCS Level II codes for supplies and medications. This is where coding accuracy determines revenue.
Undercoding selecting a lower E/M level than the documentation supports is as financially damaging as overcoding, and far more common in independent practices that lack regular coding audits. MGMA data indicates that practices lose an average of 3–5% of collectible revenue annually to undercoding alone. Over-coding creates compliance exposure under the False Claims Act.
The practical fix is a quarterly internal coding audit against documentation. It takes less than a day and typically identifies recoverable revenue opportunities within the first review.
Step 5 — Claim Submission
Clean claims claims submitted with accurate codes, correct patient information, appropriate modifiers, and complete supporting documentation are accepted on the first submission. The industry median first-pass clean claim rate is approximately 85% per MGMA. Practices below that threshold are generating rework on roughly 1 in 6 claims, which costs time and delays cash flow.
Claims move from the practice management system through a clearinghouse, which scrubs them against payer-specific rules before transmission. A clearinghouse rejection is not the same as a payer denial it means the claim never reached the payer and needs to be corrected before resubmission. Both eat into staff time and payment timelines.
Step 6 — Payment Posting
When a payer processes a claim, they send an Electronic Remittance Advice (ERA) or paper Explanation of Benefits (EOB) detailing the amount paid, any contractual adjustments, and the patient responsibility portion. Payment posting is the process of reconciling that remittance against the original claim and applying the correct accounting entries.
Underpayment identification happens at this step — or it does not happen at all. A payer reimbursing at 88% of contracted rate instead of 100% looks like a normal payment if no one checks. Across hundreds of claims per month, systematic underpayments add up to significant revenue leakage that most practices never identify because payment posting is treated as a data entry task rather than a revenue protection function.
Step 7 — Denial Management
Denied claims require identification, root-cause analysis, and where clinically and contractually justified appeal. The average U.S. physician practice has a denial rate between 5% and 15%, per CMS and commercial payer audit data. At the low end, that is manageable. At the high end, it represents a material cash flow problem.
Effective denial management is not just working the denial queue. It is identifying whether a denial pattern reflects a coding issue, a credentialing gap, a prior authorization failure, or a payer-side processing error — because each root cause requires a different fix and a different prevention protocol. Practices without a structured denial management workflow typically write off 60–70% of denied claims without appeal, leaving recoverable revenue permanently uncollected.
Step 8 — Accounts Receivable Follow-Up
Outstanding claims that have not been paid, denied, or resolved sit in accounts receivable (AR). The MGMA benchmark for total AR days in a well-managed practice is 30 to 40 days. Practices above 50 days are carrying a cash flow problem that compounds over time older claims become harder to collect and more likely to exceed timely filing windows.
AR follow-up requires systematic aging analysis: tracking what is owed by payer, by age bucket (0–30, 31–60, 61–90, 90+ days), and by denial type. Practices that treat AR as a list of things to call about rather than a structured collection workflow consistently carry higher AR days and lower net collection rates than practices with disciplined follow-up protocols.
What Good Revenue Cycle Management Looks Like for an Independent Practice
A well-managed revenue cycle in a small-to-mid-size independent practice has specific, measurable characteristics. These are the benchmarks I use when I take on a new RCM client:
| 📊 RCM Performance Benchmarks (MGMA / HFMA Standards) First-pass clean claim rate: ≥ 96% Total AR days: < 35 days Denial rate: < 5% Net collection rate: ≥ 95% of collectible charges Claim resubmission rate: < 3% Days to payment (commercial): 14–21 days average Days to payment (Medicare): 14–17 days average Source: MGMA DataDive Benchmarking, HFMA Revenue Cycle Map, CMS payment data |
If your practice is outside those benchmarks on any metric, that gap has a dollar figure attached to it. AR days of 55 instead of 35 is not an administrative inconvenience it is a specific amount of cash sitting uncollected that should be in your operating account.
Why RCM Is Harder for Small Practices — and What to Do About It
Large health systems have dedicated teams for each step of the revenue cycle. A denial specialist who does nothing but work denials. A credentialing coordinator who does nothing but manage payer enrollments. A payment posting team that reviews every remittance for underpayments.
A 3-physician practice in New York or a solo internist in Texas has none of that. They have whoever is available. And whoever is available is usually doing registration, scheduling, phones, coding, billing, and follow-up simultaneously.
That structural disadvantage is real, and it is the primary reason small and independent practices consistently underperform large health systems on every RCM benchmark not because their clinical care is worse, but because RCM is a dedicated specialty, not a task anyone can do in between other responsibilities.
The two practical options are: build internal capacity by hiring dedicated billing staff with the right credentials and management to support them, or partner with an outsourced RCM company that provides that specialized capacity without the overhead of full-time employees. I have seen both work. I have also seen both fail when the wrong choice was made for the wrong practice. If you want an honest assessment of which makes more sense for your specific situation, the team at Globill Medical Resources LLC offers a free revenue cycle review we will look at your current metrics and give you a straight answer.
The Bottom Line on Revenue Cycle Management
Revenue cycle management is not a back-office function that operates independently of clinical care. It is the financial nervous system of a practice and when it is not working, every part of the practice feels it. Physicians work harder for less money. Staff spend time chasing claims instead of supporting patients. Cash flow becomes unpredictable.
Understanding the eight steps of the revenue cycle and where your practice’s performance stands against MGMA and HFMA benchmarks is the first step toward fixing a broken cycle or protecting one that is working. If you want a clear-eyed assessment of where your revenue cycle stands today, schedule a free RCM review with the Globill Medical Resources team. We will pull the numbers, run them against benchmarks, and give you a specific picture of what is recoverable.
FAQs
What are the benefits of outsourcing RCM to Globill Medical Resources?
See what ChatGPT, Claude, and Gemini say about choosing Globill Medical Resources.


